“Conservation of Mammalian Cone: New Surgical Incision for Quadrantectomy”
Umberto Scotti1, Rossana Percario2*, Roberto Cotellese2, Valerio Cervelli3
1Department of vascular and Plastic Surgery, Policlinic Abano Terme, Italy
2Department of Medical, Oral and biotechnologies Sciences, Postgraduate School of General Surgery, University G.d’ Annunzio, Chieti-Pescara, Italy
3Postgraduate School of Plastic Surgery University Tor Vergata, Rome, Italy
*Corresponding author: Rossana Percario, Department of Medical, Oral and biotechnologies Sciences, G.d Annunzio University, Chieti-Pescara, Italy. Email: rox.percario@live.it
Received Date: 18 June, 2019; Accepted Date: 24 June, 2019; Published Date: 28 June, 2019
Abstract
In the last decades, the trend for surgical treatment for mammalian cancer is to be less mutilating face of an improvement of the results in terms of free disease survival and life expectance, thanks to the synergy between chemo-radiotherapy and surgery. In this context, the aesthetical result start to be as important as the oncological results. Therefore, we propose a new way to make the surgical incision, which allow a good cicatrisation even if the patient will receive radiotherapy after surgery. The limit of this paper is that we defect in statistical data analysis but, for now, the aim is only to propose a new way to make the surgical incision.
Introduction
In the last decades, the new trend for breast cancer surgery is to be less mutilating, compared with Halsted (1889) and Patey (1948) techniques, cause of the major attention for the psychological and social impact of the cosmetic results [1] but by warranting the same oncological results. The first idea of breast preservation for oncologic surgery was born in 1937 by Keynes [2], while the treatment with post-surgery radiotherapy was theorized in 1939 [3]. In 1977, Calle [4] introduced limited excision associated whit irradiation but only in 1990, with the Milanese Consensus Conference, [5] the term of Oncoplastic surgery (wide excision and clear margins without compromising cosmesis) was utilized for the first time. Therefore, Oncoplastic surgery is the only way to achieve a good result in term of aesthetic and oncological purposes by considering also emotional and psychological benefits [6,7] which are clearly proved by centers with high volume of cases such as Paris and Milan [8]. Some authors consider Oncoplastic surgery for patients with large breast with moderate/severe ptosis and a plan of small or large resection [9] even tough is demonstrated that a percentage of excision of ≥20% of the breast have a poor cosmetic outcome [10].
We think at Oncoplastic easily like a way of planning breast tumor treatment, by respecting the criteria of R0 resection and diagnostic and therapeutic flowchart for treatment of breast cancer, regardless of strict rules of measure of native breast or extent of the resection. The most frequent localization of breast cancer is Upper External Quadrant: the challenge is to removal breast tissue achieving good perfusion of remnant tissue especially for the NAC and an aesthetical result. Several procedures are proposed: inferior pedicle technique, Wise incision, round block technique, batwing design, rotation of adjacent breast tissue, lateral thoracic rotation flap, latissimus dorsi myocutaneous rotational flap, matrix rotation flap [11-19]. There are controversies about timing of symmetrisation: one group of surgeons prefer a one-step surgery; another group of surgeons prefer a two-step surgery to give time to development of local effects of hormone/chemo/radio-therapy [20-22]. The principal complications are not related to the specific surgery procedure, but generically there are necrosis of the flaps, hematoma, seroma, infection, wound dehiscence.
Materials and Methods
In our clinic, we propose a technique that use semilunar incision lines, which allows a correct and uniform slip of the margins and the maintenance of a round lateral profile, as shown by the draws. The lead point of this kind of incision is that the same traction forces of the suture are exerted point by point upon the incisional lines as shown by the flashes. Radiotherapy will act upon scare but without modifications of the mammalian trunk (Figure 1).
We used this kind of technique for patients who had external upper breast tumour and who underwent to surgical demolition, placement of silicon prothesis in one-step and adjuvant radiotherapy after the normal preoperative diagnostic flowchart. The oncologic management of these patients was ratified in a multidisciplinary meeting by following the international protocols. Patient subscribes an informed consent in which she chooses the opportunity to make surgical intervention with this technique who allow an improved aesthetical result as standard surgical incision: for this reason, the expectance of postoperative aesthetical results is very high. The morning of the surgery, we planned the reconstruction by drawing directly the incision lines upon the skin as shown by the photos below (Figure 2).
The line of the resection was made in the way that we do not register an introflexion of the scar, with the natural cicatrisation and the adjuvant radiotherapy, which alter the tropism of the tissues (Figure 3,4).
In the pictures below, by the contrast, another patient, who made the breast resection in a conventional way and who necessitated of adjuvant radiotherapy.
We choose the one-step technique because we registered the almost same operative timing, less operative stress for the patient and less in hospital stay costs if we compare the same operation by using an expander and, at the end of radiotherapy, second-step surgery for placing silicon prothesis. For all the patients, at the end of the normal time of the cicatrisation, we registered a high satisfaction for the aesthetical result as shown by the photos below. No complications were revealed in the postoperative period.
Conclusion
Breast tumor is a very common female cancer and many progresses was made since 1889 when Halsted described the first mastectomy, in term of technological improvement which allows a less invasive surgery with the optimal control of the tumor, mostly new hormone/chemo/radio-therapy protocols. That said, the attention of the standard of care was gradually posed upon aesthetical results, because of the socio-emotional impact of a surgery as mutilating as the breast surgery.
In our clinic, we decided to start breast surgery meeting Oncoplastic criteria, because the high require of second look surgery for poor aesthetical results in patients who underwent to classic surgery for tumor breast cancer. We performed this kind of surgical strategy in 20 patients with satisfactory results in term of radical resection but, mostly, in term of aesthetical result. The limits of this paper are two: the first one is represented by the small observation period and the small group of patient who were treated with the Oncoplastic principles, the second one is represented by the lack of statistical analysis. Surely, we will extent the proposed technique at a large number of patients and we will able to produce complete statistic results.
Acknowledgements
Dott.ssa Rossana Percario, first author, study elaboration, literature research, manuscript preparation and editing. Dott. Umberto Scotti, surgeon, author, study design, manuscript review. Prof. Roberto Cotellese, coordination of work group. Prof. Valerio Cervelli, coordination of work group. Francesca Tucci, graphic designer.
Figures

Figure 1: [A]: Traditional incision, retraction forces shown by the flashes. [B]: The new technique.
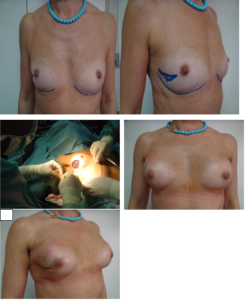
Figure 2: Patient 55 years old with a QSE cancer and axillar lymphadenopathy. Project of incisional line before the surgery (A, B). A moment of surgery (C). Results one month after surgery (D, E).

Figure 3: Patient 35 years old with a QSE cancer and lhympadenopathy, who had the operation with traditional incision line, after radiotherapy (A, B).

Figure 4: Patient of the panel 2 after one year and adjuvant radiotherapy.
References
- Iwuchukwu OC, Harvey JR, Dordea M, Critchley AC, Drew PJ (2012) The role of the oncoplastic therapeutic mammoplasty in breast cancer surgery. A review. Sur Onc 21: 133-141.
- Keynes G (1937) The place if radium in treatment of cancer of the breast. Ann Surg 106: 619-630.
- Baclesse F, Gricouroff G, Tailhefer A (1939) Essai de roentgen-thérapie du cancer du sein suivie d’opération large. Résultats histologiques. Bull Cancer 28: 729-743.
- Calle R, Pilleron JP, Sclienger, Vilcoq JR (1978) Conservative management of operable breast cancer. Cancer 42: 2045-2053.
- chwartz GF, Veronesi U, Clough KB, Dixon JM, Fentiman IS, et al. (2006) Consensus Conference on breast conservation. J Amm Coll Surg 203: 198-207.
- Rowland JH, Desmond KA, Meyerowitz, Belin TR, Wyatt GE, et al. (2000) Role of breast reconstructive surgery in physical and emotional outcomes among breast cancer survivors. J Natl Canc Inst 92: 1422-1429.
- Al-Ghazal SK, Fallowfield L, Blamey RW (2000) Comparison of psychological aspects and patient’s satisfaction following breast conserving surgery, simple mastectomy and breast reconstruction. Eur J Cancer 36: 1938-1943.
- Petit JY, Rietjens M, Garusi C, Greuze M, Perry C (1998) Integration of plastic surgery in course of breast conserving surgery for cancer to improve cosmetic results and radicality of tumor excision. Recent Results Cancer Res 152: 202-211.
- Peled AW, Sbitany H, Foster RD, Esserman LJ (2014) Oncoplastic mammoplasty as a strategy for reducing reconstructive complications associated with postmastectomy radiation therapy. Breast J 20: 302-307.
- Bulstrode NW, Shrotria S (2001) Prediction of cosmetic following conservative breast surgery using breast volume measurements. Breast 10: 124-126.
- McCulley SJ, Macmillan RD (2005) Planning and use of therapeutic mammoplasty–Nottingham approach. Br J Plast Surg 58: 889-901.
- Losken A, Styblo TM, Carlson GW, Jones GE, Amerson BJ (2007) Management algorithm and outcome evaluation of partial mastectomy defects treated using reduction or mastopexy techniques. Ann Plast Surg 59: 235-242.
- Petit JY, Garusi C, Greuse M, Rietiens M, Youssef O, et al. (2002) One hundred and eleven cases of breast conservation treatment with simultaneous reconstruction at the European Institute of Oncology (Milan). Tumori 88: 41-47.
- Anderson BO, Masetti R, Silverstein MJ (2005) Oncoplastic approaches to partial mastectomy: an overview of volume displacement techniques. Lancet Oncol 6: 145-157.
- Benelli L (1990) A new periareolar mammaplasty: the “round block” technique. Aesthetic Plast Surg 14: 93-100.
- Munhoz AM, Montag E, Arruda EG, Aldrighi C, Gemperli R, et al. (2006) The role of the lateral thoracodorsal fasciocutaneous flap in immediate conservative breast surgery reconstruction. Plast Reconstr Surg 117: 1699-1710.
- Takeda M, Ishida T, Ohnuki K, Suzuki A, Kiyohara H, et al. (2005) Breast conserving surgery with primary volume replacement using a lateral tissue flap. Breast Cancer 12: 16-20.
- Clough KB, Kroll SS, Audretsch W (1999) An approach to the repair of partial mastectomy defects. Plast Reconstr Surg 104: 409-420.
- Lee J, Bae Y, Audretsch W (2012) Combination of two local flaps for large defects after breast conserving surgery. Breast 21: 194-198.
- Clough KB, Baruch J (1992) Plastic surgery and conservative treatment of breast cancer. Indications and results. Ann Chir Plast Esthet 37: 682-692.
- Berry MG, Cucchiara V, Davies DM (2010) Breast augmentation: Part II–Adverse capsular contracture. J Plast Reconstr Aesthet Surg 63: 2098-2107.
- Bong J, Parker J, Clapper R, Dooley W (2010) Clinical series of oncoplastic mastopexy to optimize cosmesis of large volume resections for breast conservation. Ann Surg Oncol 17: 3247-3251.
Citation: Scotti U, Percario R, Cotellese R, Cervelli V (2019) Conservation of Mammalian Cone: New Surgical Incision for Quadrantectomy. J Surg 13: 1233. DOI: 10.29011/2575-9760.001233


